Why Immunocompromised Patients Face the Highest Risk
A healthy adult inhales an estimated 100 to 1,000 Aspergillus spores every day in tropical Singapore, and clears every one of them silently. Pulmonary alveolar macrophages identify and destroy spores within hours; neutrophils mop up any hyphae that begin to germinate. The system is so robust that aspergillosis is virtually unheard of in healthy people.
That defence collapses when neutrophil counts drop below 500/μL (severe neutropenia), when corticosteroids suppress macrophage function, or when calcineurin inhibitors used after transplant prevent T-cell recognition of fungal antigens. Once a single spore germinates inside the lung, hyphal growth is angioinvasive — the fungus drills into pulmonary blood vessels, causing infarction, haemorrhage and dissemination to brain, sinuses, kidneys and skin within days.
The World Health Organization's 2009 guidelines on indoor dampness and mould explicitly identify immunocompromised individuals as the population requiring the lowest possible spore exposure. The Institute of Medicine's 2004 report Damp Indoor Spaces and Health reaches the same conclusion. There is no safe threshold for this group — only "as low as reasonably achievable."
Highest-Risk Patient Groups
- Acute leukaemia — particularly during induction and consolidation chemotherapy when neutropenia lasts 14–28 days
- Allogeneic stem-cell / bone marrow transplant — the highest-risk group globally; aspergillosis incidence 5–15% with mortality up to 90% if cerebral
- Solid organ transplant — lung (highest), heart, liver, kidney recipients on tacrolimus, cyclosporine or mycophenolate
- HIV with CD4 count below 200 — particularly when also receiving steroids for PCP prophylaxis
- Long-term high-dose corticosteroids — prednisolone above 20 mg/day for more than 3 weeks
- Biologic therapy — anti-TNF (infliximab, adalimumab), anti-IL-6 (tocilizumab), JAK inhibitors, anti-CD20 (rituximab), anti-BTK (ibrutinib)
- Severe COPD on chronic inhaled or oral steroids — at risk of chronic pulmonary aspergillosis
- Cystic fibrosis — at risk of allergic bronchopulmonary aspergillosis (ABPA)
- Diabetes mellitus, poorly controlled — at risk of mucormycosis from Rhizopus species
- Severe burns and ICU patients on broad-spectrum antibiotics
Singapore-Specific Exposure Profile
Singapore's climate is essentially designed for fungal growth. Average outdoor relative humidity is 84% year-round, and indoor humidity in HDB and condo flats typically sits between 70% and 90% unless aggressively dehumidified. Aspergillus fumigatus, A. niger, A. flavus, Penicillium, Cladosporium and Stachybotrys chartarum are all well-documented as endemic indoor isolates in Singapore housing.
Three exposure routes are particularly dangerous for immunocompromised households:
- Air-conditioner biofilm — split-unit evaporator coils run at the dew point, accumulating Cladosporium and Aspergillus biofilm within 6–12 weeks of last servicing. Each compressor cycle aerosolises spores directly into the breathing zone.
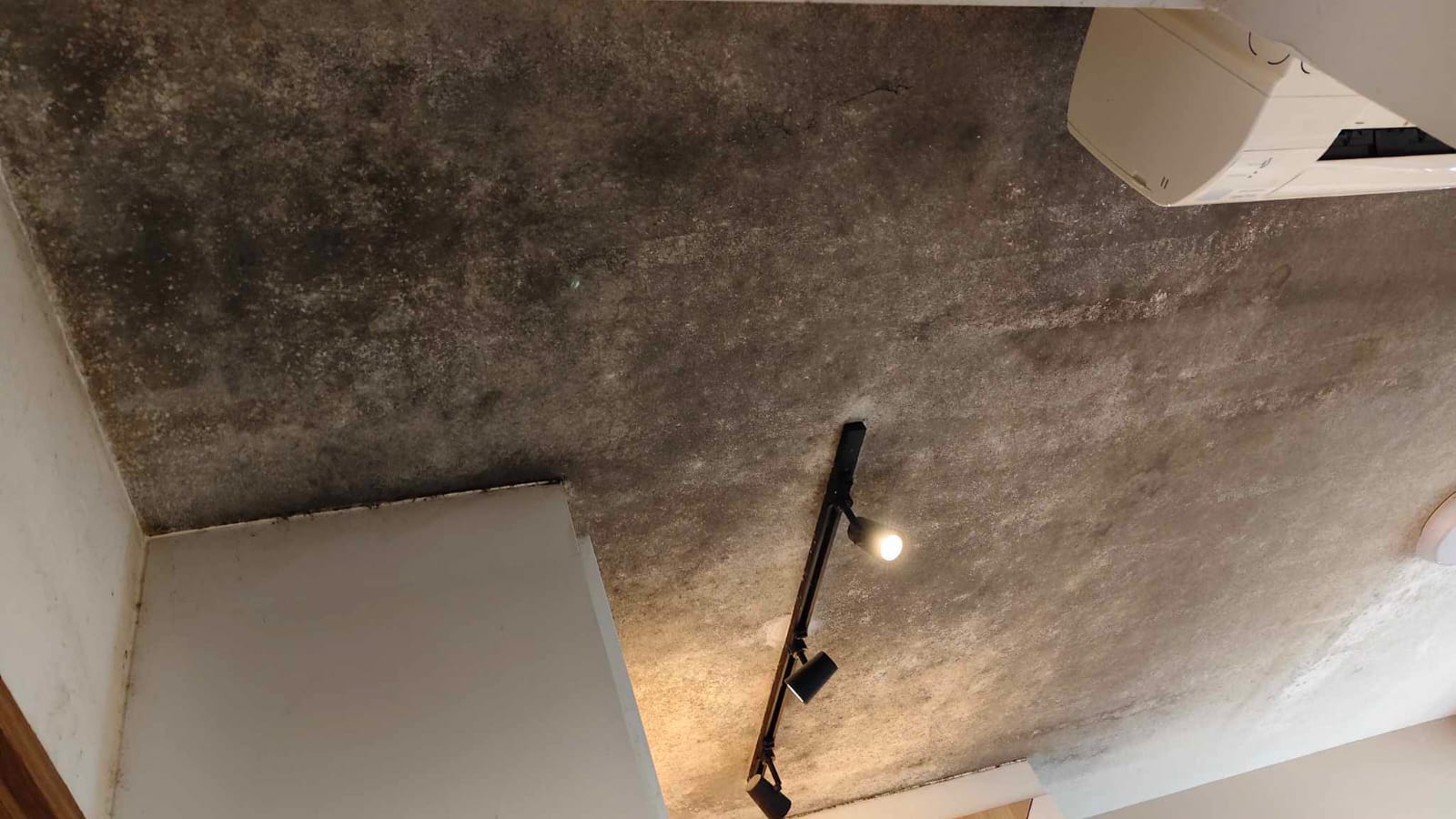
- Bomb-shelter and store-room wall cavities — concrete walls without proper vapour barriers harbour hidden Stachybotrys colonies that release spores into adjacent bedrooms whenever the door is opened.
- Bathroom-adjacent bedroom walls — moisture migration through unsealed grout creates colonies on the bedroom side of the shared wall, often invisible until paint blistering appears.
The monsoon transitions in November–January and June–July produce humidity spikes that double indoor spore counts within 48 hours. Patients about to begin a chemotherapy cycle during these months should consider a pre-cycle environmental audit.
Acute Symptoms & Red Flags
Invasive aspergillosis is notoriously hard to diagnose early because symptoms mimic bacterial pneumonia. For an immunocompromised patient living in a home with any visible mould, the threshold for suspicion must be very low. Seek same-day medical attention if any of these appear:
- New fever above 38°C unresponsive to broad-spectrum antibiotics within 72 hours
- Pleuritic chest pain (sharp pain on deep breath)
- Haemoptysis (coughing blood, even small amounts)
- New shortness of breath at rest
- Sinus pain, facial swelling, or black eschar inside the nostril (mucormycosis red flag)
- New visual disturbance or unilateral facial weakness (CNS dissemination)
- Skin lesions with central necrosis (cutaneous dissemination)
Do not wait for the next clinic appointment. Bring a photograph of any visible household mould to the emergency department — it materially changes the empirical antifungal decision.
Long-Term Health Consequences of Continued Exposure
Even when a single acute episode is survived, repeated low-dose exposure has measurable long-term consequences in this population:
- Chronic pulmonary aspergillosis (CPA) — cavitating lesions that mimic tuberculosis on CT, requiring 6 months to lifelong itraconazole or voriconazole, with progressive fibrotic loss of lung volume
- Allergic bronchopulmonary aspergillosis (ABPA) — IgE-mediated airway inflammation causing fixed airflow obstruction and central bronchiectasis
- Hypersensitivity pneumonitis — granulomatous interstitial lung disease that can become irreversible after months of exposure
- Mycotoxin bioaccumulation — ochratoxin A, gliotoxin and aflatoxin exposure has been associated in the clinical literature with persistent fatigue, cognitive impairment ("brain fog"), peripheral neuropathy and accelerated immunosenescence
- Increased post-transplant rejection rates — sub-clinical fungal infection appears to potentiate alloimmune response in solid-organ transplant cohorts
- Reduced 5-year survival — haematology cohorts with documented household mould exposure show measurably lower 5-year overall survival even after the acute infection is treated
The cumulative picture is that mould exposure does not stop being a problem once an acute infection is controlled. It continues to subtract years of life and quality of life across the survivorship period.
Pre-Treatment Home Audit — What to Check
Ideally performed 2–4 weeks before chemotherapy or transplant induction. Either DIY using the checklist below, or book a professional inspection.
- All bathroom ceilings, especially the corner farthest from the exhaust fan
- Wardrobe back walls (pull wardrobe 30 cm from the wall, look and smell)
- Aircon evaporator coil — open the front cover and inspect the fins; black film = biofilm
- Bomb shelter walls, ceiling and door seal
- Bedroom walls adjacent to bathroom or kitchen (look for paint blistering or hairline cracks)
- Under-sink cabinets in kitchen and bathroom
- Window frames and the wall directly below window air-con units
- Behind any wallpaper that was applied over previous paint
For BMT or solid-organ transplant candidates we recommend going further: spore-trap air sampling in the patient's bedroom and a borescope inspection of any wall cavity that was previously affected by water damage. Hidden mould accounts for an estimated 70% of total household contamination.
Hospital-Grade Remediation Protocol for Immunocompromised Households
Standard residential mould removal is not appropriate for this group. The work must follow infection-control principles closer to a hospital construction-site (ICRA Class III/IV) than to a typical home renovation:
- Patient relocated for the entire treatment day plus a clearance period — typically 4–6 hours after work ends
- Negative-pressure containment — work zone sealed with 6-mil polyethylene; HEPA-filtered air scrubber maintains 4–6 air changes per hour at negative pressure to the rest of the home
- Botanical sporicidal antimicrobials only — thymol and citric-acid based blends that break down to water and CO2; no quaternary ammonium, no bleach, no chlorine dioxide (these leave reactive residues that worsen chemo-induced mucositis)
- HEPA-vacuum + wet-wipe protocol — every surface in the work zone, then 1.5 m beyond the containment
- Substrate decision — porous materials with deep colonisation (drywall, ceiling board, gypsum) are removed and replaced rather than cleaned, in line with IICRC S520 and IOM 2004 recommendations
- Post-treatment air sampling — Andersen impactor spore-trap inside and outside the containment; written clearance report comparing indoor to outdoor counts before re-entry is authorised
- HVAC isolation — air-conditioning to the affected zone shut down throughout the work and the coil itself cleaned separately if implicated
- Documentation pack for medical records — pre/post photographs, antimicrobial product safety datasheets, air sampling results, technician PPE log
Coordination with Your Care Team
The most useful thing we can do, beyond the physical work, is provide your specialists with documentation that integrates into your clinical record. We routinely send the post-treatment clearance report directly to oncologists, transplant coordinators, infectious-disease consultants, paediatric haematologists and respiratory physicians at all major Singapore hospitals on request.
Specific items we can prepare on request:
- Pre-treatment hazard assessment letter for insurance pre-authorisation
- Antimicrobial product MSDS confirming residue-free profile suitable for residency by neutropenic patients
- Post-treatment air sampling report with quantified spore counts and species identification
- Re-entry recommendation letter with specific timing
- Six-month follow-up re-inspection report for transplant survivorship clinics
If your specialist wants to speak with our project lead before scheduling, we are happy to arrange a 15-minute call at no charge.
Related Reading
Frequently Asked Questions
How urgent is mould removal before chemo?
Ideally complete remediation 7–14 days before the patient enters cytopenia (neutrophil count below 500). If chemo is already underway and mould is discovered, immediate remediation with full patient relocation is the standard protocol. Coordinate timing with your oncologist — never delay treatment, but never start a high-dose cycle in a known mould-contaminated home.
Is HEPA filtration alone enough?
No. HEPA reduces airborne load temporarily but does not eliminate the spore source. As long as the colony is alive on a damp substrate it will keep producing spores faster than a portable purifier can clear them. For neutropenic, transplant or biologic-therapy patients, source removal is non-negotiable; HEPA is a supplement, not a substitute.
Can my caregiver be in the room during treatment?
Yes, with the P100 respirator and Tyvek suit we provide. The patient is fully relocated for the day. Re-entry for the patient occurs only after post-treatment air sampling shows clearance, typically 4–6 hours after work ends. Caregivers may re-enter sooner once visible spore-load work is complete.
Will my health insurance cover this?
Some Integrated Shield Plans, critical-illness riders and home insurance policies cover environmental remediation when medically indicated. Bring a written letter from your specialist stating the medical necessity; we provide itemised invoices, antimicrobial product datasheets, and post-clearance air sampling reports suitable for insurance submission.
What is invasive aspergillosis and why is it so dangerous?
Invasive aspergillosis is when Aspergillus fumigatus spores germinate inside lung tissue instead of being cleared by alveolar macrophages. The hyphae invade blood vessels, causing tissue infarction and disseminated infection to the brain, sinuses and skin. Mortality is 30–50% with treatment and approaches 90% in stem-cell transplant patients with cerebral involvement. It is the leading invasive fungal infection in haematology wards globally.
Are botanical antimicrobials safe for chemo patients to be near?
Yes — that is precisely why we use them. Quaternary ammonium compounds and chlorine-based biocides leave residues that can trigger reactive airway disease in patients with chemo-induced mucositis. Our botanical sporicidal blends (thymol and citric-acid based) break down into water and CO2, leaving no residue. Patients can re-enter once airborne particulate counts return to baseline.
How do I know if there is hidden mould before treatment starts?
Visible patches are only 20–30% of the contamination in a typical Singapore HDB. Hidden colonies live behind wardrobes against external walls, inside aircon evaporator coils, under bathroom floor tiles, and in bomb-shelter wall cavities. Pre-chemo we recommend a moisture-meter and borescope inspection of all known wet zones, plus optional spore-trap air sampling for patients about to undergo BMT or solid-organ transplant.
What is the long-term lung impact if exposure continues?
Chronic low-grade Aspergillus exposure in immunosuppressed patients can progress to chronic pulmonary aspergillosis (CPA) — cavitating lung lesions that mimic tuberculosis, require 6+ months of antifungal therapy, and cause permanent fibrotic loss of lung volume. Mycotoxin exposure has also been linked in clinical literature to persistent fatigue, cognitive dysfunction, and accelerated immune senescence even after the acute infection resolves.
Free WhatsApp Inspection. No hard sell.
Send us a photo of your mould — most cases don't need a paid on-site inspection. We'll tell you honestly if a visit is needed, or quote you directly. Transparent pricing, zero obligation.
Free WhatsApp Inspection Call +65 8751 5146 On-Site Inspection (if needed)No hard sell. Transparent pricing. Reply within working hours.